
Side Quest: The Cass Report - Why the Reaction is 'Toxic'
An Idiot's Guide to Understanding Why People Reject the Report on Gender Identity Services for Children and Young People

The general public often overlooks the trans debate, engaging only superficially with media coverage before moving on with their lives, without a strong stance on either side. Today, James O’Brien discussed the Cass Report on his LBC show. The discussion was characteristically valuable, but there was an element of ‘bothsidesism’, the idea that both the anti-trans and pro-trans sides were, more or less, equally volatile and aggressive.
One of the major issues for those who come to the ‘trans debate’ from a position of personal indifference, is that while they ‘breath in’ a lot of the sensationalistic scaremongering promoted in the mainstream media, they are never exposed to the details that help to explain the reactions of the ‘pro-trans side’ of the supposed debate. The Cass Report is a case in point.
In this post, I’ll help to explain why many people rejected the Cass Report without even having read the final report issued today and explain why it is not simply a matter of ‘not liking’ the results of an independent investigation.
Background and Context
In September 2020, the NHS announced that Dr Hillary Cass had been appointed to lead an independent review into gender identity services for children and young people, for the National Institute for Health and Care Excellence (NICE). Such reviews are not uncommon, however the background to the announcement was anything but common. The review was established in the context of rising demand for gender identity services, alongside profound concerns about the quality of care provided and rising transphobia in the UK. Many felt that the motivation behind the commissioning of the review was, in part, political. However, it also followed on from a pretty damning CQC report into the NHS Gender Identity Development Service run by the Tavistock and Portman NHS Foundation Trust. Many trans people hoped that the review might lead to improvements in the quality of trans healthcare.
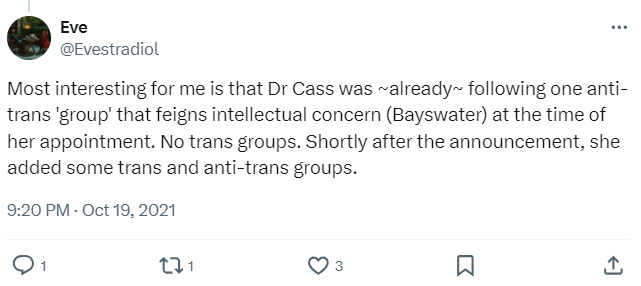
Concerns about Dr. Cass's impartiality surfaced swiftly, evidenced by her social media affiliations with groups considered by many as transphobic. While Dr Cass later claimed that she followed people “on all sides of the debate”, Twitter detectives claimed that the only group she followed prior to her appointment was the trans-sceptic Bayswater Support, and many pro-trans groups were only followed after this controversy emerged. Dr Cass also followed the LGB Alliance, based on the notorious Tufton Street and the anti-trans pressure group, Transgender Trend. This discovery cast a long shadow over the review's claimed neutrality.

In April 2021, the Cass Review website was launched. The website’s governance section made it clear that transgender people had been deliberately excluded from the governance of the review. The Cass Report’s team had, apparently, decided that being trans made one incapable of objectivity - even if a transgender individual held expertise in areas like clinical and research ethics, medical law or paediatric medicine. This decision was akin to excluding pregnant women, or formerly pregnant women from the governance of a project designed to review maternity services. Just as such a decision would be regarded as sexist, the Cass team’s decision was widely regarded as transphobic.
In 2022, the interim review faced stringent criticism from experts within the transgender healthcare community. The report claimed that there was a need for more long term data to assuage fears around the use of hormonal interventions. While Cass acknowledged that there was no prospect of filling the supposed evidence gap, the interim report claimed that there was a need to develop a professional consensus on the way to proceed.
Critics, pointing to a wealth of empirical research and clinical evidence already affirming the positive impact of these interventions, challenged the review for overlooking existing substantiation of the treatments' efficacy. They also pointed out that such consensus already exists outside the UK and that The American Academy of Pediatrics, the Endocrine Society, and the World Professional Association for Transgender Health have all endorsed the use of these hormonal treatments in gender diverse young people. However, Cass team instead seemed to want to develop guidelines on the basis of “conceptual agreement” and “shared understanding” among all ‘interested parties’ - which seemed to include those who viewed transgender identity as inherently pathological or sinful.
The final report's reliance on the GRADE system to evaluate research further compounded the controversy. Critics argue this methodology is ill-suited for transgender healthcare interventions, potentially disregarding or downgrading valuable evidence due to rigid standards unachievable in this context.
Using the grade system, research findings were downgraded due to a lack of blinding and/or the absence of a control group. While such ratings are in line with standard practice when using the GRADE system, critics pointed out that it is virtually impossible to blind someone taking hormones, as they will notice things like the development of breasts or facial hair. Similarly, Randomised Control Trials, the gold standard according to the GRADE system, are regarded as unfeasible and unethical when investigating hormonal interventions as disallowing puberty suppression results in the irreveersible development of secondary sex characteristics. The Cass team also chose to exclude any study not reported in English, single case research designs and systematic reviews. In effect, when the research team chose to use the GRADE system, they knew that gender affirming care interventions could never meet its criteria to be regarded as evidence-based.
While one might be willing to dismiss this choice as a methodological preference that positions experimental robustness ahead of utility, the final report also featured several claims and recommendations that were entirely speculative. The report claimed that “it is possible that social transition in childhood may change the trajectory of gender identity development for children with early gender incongruence,” despite the fact that none of the evidence included within the report supports this idea. It also made somewhat bizarre claims about trans-history, claiming that “For many centuries transgender people have been predominantly trans females, commonly presenting in adulthood.” This highlights the inherent contradiction in the Cass Report: it sets unattainably high criteria for validating gender-affirming care while applying far less rigorous standards to its own recommendations.
In sum, the Cass Report has faced rejection for several reasons: perceived political motivations behind its commissioning, concerns about Dr. Cass's impartiality due to her affiliations with groups seen as transphobic, the exclusion of transgender individuals from the review's governance while simultaneously engaging with transphobic lobby groups, its failure to consider international guidance and criticism from transgender healthcare experts over its methodology and conclusions. Critics argue that existing consensus and evidence supporting hormonal interventions have been overlooked, and some claims made in the report are seen as speculative and unsupported by included evidence.
Transgender Anger
The coverage of the Cass Report in the media has been overwhelmingly positive. None of the coverage I’ve seen or heard today covers any of the concerns noted in the previous section. It is remarkable that a report that primarily affects the transgender community has not centred their views or concerns.
Dr. Cass, in conversation with The Guardian, positioned herself as an impartial clinician caught in a maelstrom she characterised as "toxic, politicised, and ideological." Yet, under her leadership, the report extended equal legitimacy to groups like the LGB Alliance and Stonewall, a move seen by many as equating transphobic lobby groups with LGBT self-advocacy groups. Furthermore, the decision to exclude transgender individuals from the project's governance underscores an approach that can only be seen as transphobic.
The choice of a research grading system by Cass’ team, known to undervalue the types of designs used to evaluate hormone therapy interventions from the outset, further emphasises this bias. Describing the supporting evidence for hormone interventions as "poor" after using a system that predisposes to such a conclusion not only undermines the commitment to evidence-based medicine but also suggests a hypocritical stance. Advocating for alternative approaches without a solid evidence base, while dismissing gender-affirming interventions for purported lack of evidence, raises significant concerns about the consistency and integrity of the report's conclusions.
When one is aware of these factors, as many in the trans community are, the ‘toxicity’ of the comments directed towards the Cass team and the report’s findings becomes more understandable. The approach taken by Dr Cass and her colleagues cannot be justified. It was unarguably, at times, transphobic in its approach and it is now being used to justify the withdrawal of gender affirming care, recognised as vital by transgender healthcare experts across the globe.
And if the Cass Review was the only incident of transphobic commentators and institutions being presented as victims of ‘toxicity,’ perhaps some angry reactions might still be regarded as over the top. But the Cass case is not exceptional. It’s the standard way in which the ‘trans debate’ is conducted. Transgender voices are suppressed while anti-trans prejudice is normalised.
Wouldn’t you be angry too?